Definition of Keratoconus:
Keratoconus is a corneal disorder where central or paracentral cornea undergoes progressive thinning causing irregular astigmatism, which is progressively increasing.
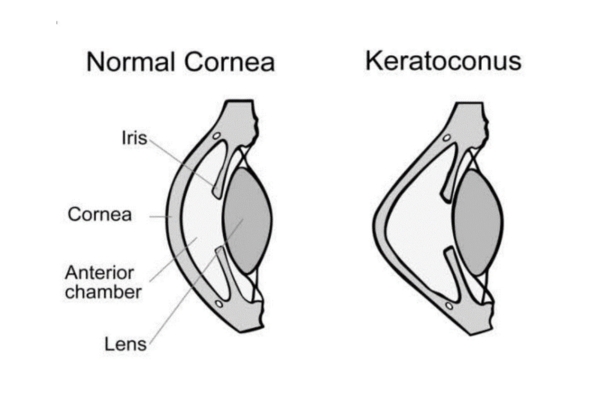
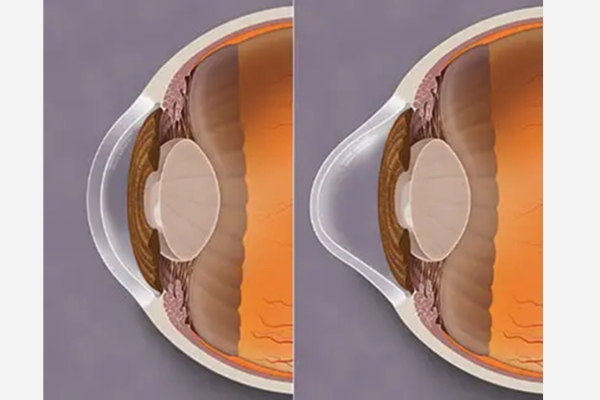
In healthy Eye, cornea is the transparent, dome-shaped window at the front of your eye. It has power and it helps in focusing light into your eye.
In Keratoconus the cornea thins out and bulges like a cone, changing the shape of the cornea, causing defocusing of light rays out of retina. Patient develops Myopic Astigmatism, sometimes with Myopia and it will keep on progressing.
As a result, vision is blurry and distorted, making daily tasks like reading or driving difficult.
Symptoms in early stages:
- Mild blurring of vision
- Slightly distorted vision, where straight lines look bent or wavy
- Increased sensitivity to light and glare
- Eye redness or swelling of lid
- Need Glass prescription or Contact lens (Soft and RGP) to improve quality of vision
Symptoms in later stages:
- More blurry and distorted vision
- Increased Myopia (Near-sightedness) or Myopic Astigmatism – difficulty in vision especially distant, but near also can be distorted
- Frequent change in eyeglass/contact lens prescriptions
- No end point vision correction with Glasses- despite giving full correction or sometimes correction is difficult because of too much distortion over the cornea.
- Inability to wear contact lenses- They may no longer fit properly and they are uncomfortable
Diagnosis of Keratoconus:
Thorough and complete Eye Examination which includes
- Vision and glasses check-up- Generally patients have Compound Myopia (Myopia/Near-sightedness with Myopic astigmatism) which is progressing
- Retinoscopy- Scissoring Reflex
- Rizutti’s sign-
- SLE- Lid tightness, Papillae in upper tarsal conjunctiva/Allergy in the eye, Cornea Examination- Fleischer Ring, Vogt’s striae, in late stages, Munson’s sign and breaks in Descemet’s membrane or scar in the cornea
- Keratometry/Computerized Topography/Computerized Tomography/Ultrasound pachymetry- Important parameters include- K reading and Thickness of the cornea along with astigmatism and irregularity over cornea. Inferior (more common)/Central steepening. Skewed axis, elevated Keratometry values, thinning of cornea over steepest cornea (Cone of Keratoconus)
- Corneal thickness mapping
Differential Diagnosis:
- Pellucid Marginal Degeneration
- Keratoglobus
- Contact lens induced Corneal warpage
- Post Laser Refractive Surgery Corneal Ectasia
Primary prevention of Keratoconus:
- No preventive strategy has been proven effective to date
- Eye rubbing and pressure over eye- can cause progression of Keratoconus- education about them especially to Kids
- Avoidance of allergens and treatment of Ocular surface disease may help to decrease eye irritation and therefore rubbing
Treatment of Keratoconus:
There is no medical treatment of Keratoconus. But depending on other co-existent situation, medical treatment gives not only relief, but will also have impact on progression of Keratoconus.
Vision improvement is most important help, extended to patients, and is very effectively done, either by glasses or contact lens.
With contact lenses, especially specialised ones, the quality of vision improves dramatically in case of Keratoconus.
- Mild symptoms- corrected with Glasses
- Mild to Moderate progression- Contact lens (RGP Contact Lenses/ROSE K/SCLERAL contact lenses) trial- If vision is not improving with glass or very high astigmatism to improve quality of vision
- Medical treatment- Associated allergic conditions should be attended properly
- Atopic or Vernal Conjunctivitis- Topical antihistamines, mast cell stabilizers, or Anti-inflammatory/Immunomodulatory treatments such as Topical Steroids, Cyclosporine, Tacrolimus or Lifitegrast
- Sleep Apnea- find out sleep habits, sleep studies, CPAP mask if necessary
Surgical treatment in case of progression of Keratoconus
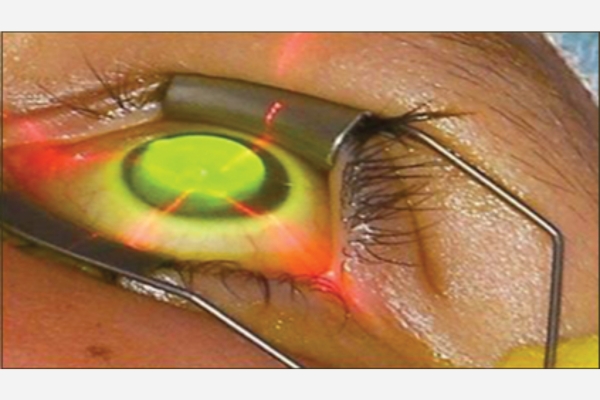
- Collagen cross-linking (C3R/CXL)– It is commonly performed procedure in case of progression of Keratoconus
- The primary purpose of cross-linking is to halt the progression of ectasia, so it should not be done unless and until, progression of Keratoconus is recorded. As it has significant future ramifications’ like, extreme flattening of Cornea, melting of Cornea etc, though not common.
In C3R procedure– Cornea is exposed/treated with UV light in presence of Riboflavin (Photosensitizer) solution. UV rays strengthen bond between corneal stromal fibres and thus strengthen the corneal biomechanics to stop the progression of Keratoconus.
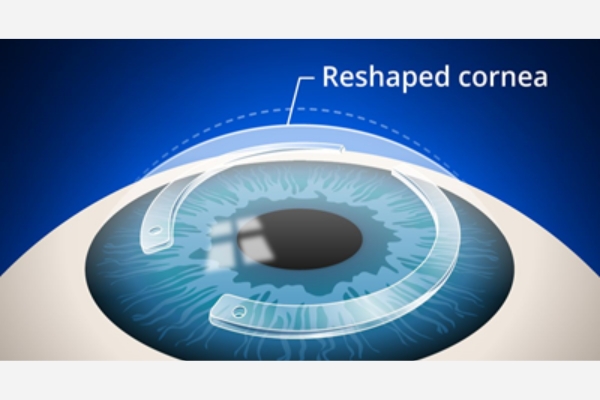
Intacs/ICRS (Intrastromal Corneal Ring Segments)/CLAIRS:
Intacs is a transparent curved plastic ring segments, surgically positioned into the corneal stroma, to treat extreme Keratoconus by flattening its irregular, conelike shape.
CLAIRS (Corneal Allogenic Intrastromal Ring Segments)- uses donor corneal tissue to reshape and support cornea in extreme Keratoconus.
It helps to flatten the curvature of cornea which is protruding/bulging in Keratoconus and that is how it improves the vision. Most of the time, it is performed along with Collagen Cross-linking.
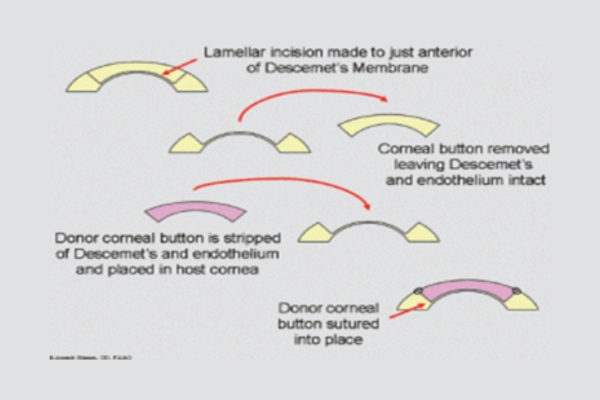
Corneal Transplant – Deep Anterior Lamellar Keratoplasty (DALK)
Corneal transplant means, diseased cornea is replaced with healthy donor cornea tissue. In DALK procedure cornea is partially (Anterior part) replaced with donor cornea. It is performed when there is extensive bulging of the cornea or scar formation over the cornea. Advantage of DALK surgery over PK, is, as patient’s endothelial layer is preserved, chances of rejection of graft dramatically decreases.
Extreme case of Keratoconus- Penetrating Keratoplasty (PK)
Total Keratoplasty means whole diseased cornea is replaced with healthy donor cornea. In extreme cases, especially where DALK cannot be done, the PK procedure is performed.
- With early diagnosis and intervention like treatment of Allergy in the eye, education on no rubbing, can effectively holt or slow down the progression of Keratoconus
- Once stable, majority of patients are comfortable with glasses and contact lenses, in mild to moderate cases. The significant vision is retained with spectacle lenses or contact lenses throughout the life in majority of patients
- In case of documented progression, Corneal Collagen Cross-linking (CXL/C3R), is performed.
- Intacs/ICRS/CLAIRS- helps in limited cases, basically helps in reducing astigmatism, thus helps in improving quality of vision. Generally performed with CXL/C3R
- Keratoplasty- DALK or PK – Though rehabilitate them well, but requires long term therapy with Steroids with long term follow up
- “Progression” of Keratoconus- has been reported even after corneal surgery, it is still not clear how common or to what extent this can occur. Also, there are multiple factors which plays crucial role here.
- Ectasia, induced by Laser Refractive Surgery treated with same way like Normal Keratoconus
Regular follow-up with Cornea Expert is very important